For Patients
Uterine myoma
Symptoms
The uterine myoma is a benign tumor derived from the smooth muscles constituting the uterus and frequently develops in women from relatively young ages to postmenopausal ages. It does not cause any particular symptom and is often found by chance during medical examinations.
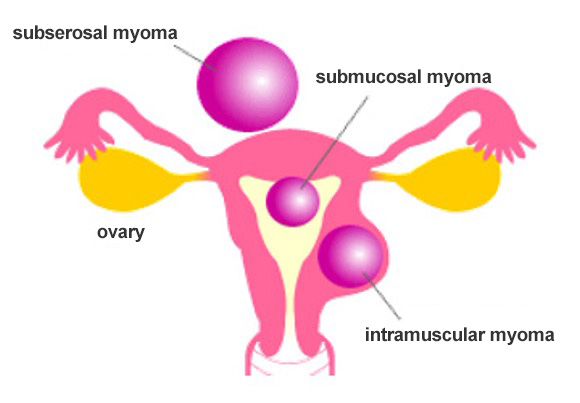
Uterine myomas are classified into subserosal, intramuscular, and submucosal myomas depending on the site of occurrence (Fig. 1). It can also cause bleeding, necrosis, calcification, and degeneration such as edema-like degeneration.
Symptoms include menorrhagia, prolonged menstruation, menstrual pain, palpable abdominal mass, and anemia. When the uterine myoma grows, it compresses surrounding organs, causing symptoms such as frequent urination, difficult urination, constipation, and low back pain. It sometimes causes infertility and premature birth as well. The intensity of symptoms depends on the location, size, and number of uterine myoma.
Subserosal myoma is less likely to cause symptoms such as menstrual pain, menorrhagia, and prolonged menstruation, but can cause severe pains due to pedicle torsion. Compared to myomas in other parts of the body, submucosal myomas are more likely to cause symptoms such as menorrhagia, prolonged menstruation, and menstrual pain from younger ages, and also prone to cause anemia.
Figure 1
Diagnosis
Diagnosis is made by combining the findings from multiple tests such as pelvic examination, ultrasonography, and MRI examination if necessary. Uterine sarcoma, which is rare but one of the malignant tumors of uterine origin, should also be suspected when the imaging findings are not typical of uterine myoma, or when the tumor enlarges after menopause.
Treatments
When the uterine myomas are asymptomatic and are not very large (i.e., smaller than or equal to the size of a fist), receiving regular examinations is enough, requiring no particular treatments in most cases. However, treatments should be considered when the tumors are large with significant tendency to enlarge or when symptoms are problematic in life.
- Pharmacotherapy
- Pseudomenopause therapy: a treatment that uses a drug called gonadotropin-releasing hormone (GnRH) agonist or antagonist that suppresses the production of female hormone, estrogen, in the ovaries to reduce myoma, and is used for women just before menopause or to avoid surgery due to serious complication. GnRH agonists are given by injection once a month or as nasal drops twice a day, while GnRH antagonists, which were recently approved, are given orally once a day. They are also effective as pretreatments for uterine myomectomy, which removes only myomas. The symptoms improve because of amenorrhea during the treatment. Menopause-like symptoms are observed because ovarian functions are suppressed. Long-term use of 6 months or longer cannot be made due to adverse effects such as bone loss. Its discontinuation results in the re-enlargement of uterine myoma and the recurrence of symptoms.
- Symptomatic treatment: a treatment with the main purposes of relieving symptoms such as menorrhagia, prolonged menstruation, and menstrual pain due to uterine myoma.
(1) Iron preparation, which is prescribed for anemia due to menorrhagia or prolonged menstruation.
(2) Non-steroidal anti-inflammatory drug, which is administered for controlling the pains associated with dysmenorrhea such as menstrual pains.
(3) Low-dose estrogen/progestin combination drug (LEP preparation) aimed at mitigating dysmenorrhea. It does not reduce the sizes of the uterine myoma themselves. It can cause serious adverse effects such as thromboembolism in rare cases.
(4) Intrauterine luteal hormone release system, in which a device that continuously releases luteal hormone is inserted into the uterus to suppress the growth of the endometrium to make it thinner thereby mitigating menorrhagia and dysmenorrhea. It does not reduce the sizes of the uterine myoma themselves. It requires regular replacement.
- Surgery
- Total hysterectomy: A choice of treatments when there is no wish or plan to become pregnant without the need for preserving the uterus. Choices are laparotomy and laparoscopic surgery, as well as vaginal procedures involving only the operations from vagina. Laparoscopic surgery has recently become common in gynecological surgery. Laparoscopic total hysterectomy is commonly used in consideration of the sizes of the lesions and the presence of movability. Total vaginal hysterectomy may be chosen when the patient has a history of vaginal delivery, the uterus is highly movable, and intra-abdominal adhesions are not expected; however, it is decreasing in association with the dissemination of laparoscopic surgery.
- Uterine myomectomy: a surgical procedure often used for women in reproductive ages who wish or plan to become pregnant. It hollows out only the part of the uterine myoma, while preserving the uterine body that is necessary for pregnancy. Laparotomy or laparoscopic surgery is chosen in consideration of the location, size, and number of the tumor. Uterine myoma can recur because this procedure leave the uterus itself.
- Hysteroscopic uterine myomectomy: used for less large submucosal myomas that protrudes into the uterine cavity. The size of the uterine myoma and the extent of its protrusion into the cavity determine whether it can be used.
- Hysteroscopic endometrial ablation (microwave endometrial ablation, MEA): a procedure involving the insertion of an apparatus into the uterus to necrotize the endometrium with microwaves. Since it does not treat uterine myomas themselves, diminution of uterine myoma cannot be expected. It is minimally invasive and can lead to the relief of symptoms such as menorrhagia; however, it cannot be used when the patient is expecting pregnancy in the future. In addition, it may not be indicated depending on the condition of the uterine cavity and uterine wall.
- Uterine artery embolization (UAE): a procedure to shrink uterine myoma by inserting a catheter into a blood vessel through the inguinal region, stuffing the uterine artery with vascular embolizing substances under fluoroscopy, and blocking blood flow. It can alleviate symptoms, but can cause complications such as post-treatment pains, infection, fever, fatigue, and decreased ovarian functions. It has also been reported that the capability of becoming pregnant can decrease. It is chosen when surgery is difficult due to complications or urgent bleeding control is required; therefore, it is not often used commonly.
Each treatment has its strengths and weaknesses; therefore, the treatment to use is decided by considering age, plan to become pregnant in the future, as well as the size, location, and number of uterine myoma, along with the presence of adhesions. We recommend that you get fully explained about these by your doctor and well convinced before receiving any treatment (Table 1).
Table 1 Treatment of uterine myoma
| Uterine myoma | No treatment required | Follow-up | |||
|---|---|---|---|---|---|
| Treatment required | Pharmaco- therapy |
Symptomatic treatment | ・Iron preparation ・Non-steroidal anti-inflammatory drug ・Low-dose estrogen/progestin combination drug (LEP preparation) ・Intrauterine progesterone release system |
||
| Pseudomeno- pause therapy |
・GnRH (gonadotropin-releasing hormone) agonist and antagonist | ||||
| Surgery | Wish to become pregnant | ・Uterine myomectomy ・Hysteroscopic uterine myomectomy |
|||
| No wish to become pregnant | ・Total hysterectomy ・Uterine myomectomy ・Hysteroscopic uterine myomectomy ・Hysteroscopic endometrial ablation (MEA) ・Uterine artery embolization (UAE) |
||||
Because uterine myoma is benign, patients often do not require any treatment. Treatment may be considered if any symptoms are degrading the quality of life. However, receiving treatments such as surgery does not always eliminate symptoms. As it rarely enlarges after menopause with worsened symptoms, you should consult with your doctor about the need for hospital visits and treatments.
[In case of complication of pregnancy with uterine myoma]
Uterine myoma may be found only after being aware of pregnancy. Pregnancy may proceed normally without any problem even if complicated with uterine myoma, whereas preterm birth, degeneration of uterine myoma, labor disorders, or postpartum bleeding may occur. Conservative therapy and follow-up are often performed for uterine myoma during pregnancy. Please discuss well on the necessity and safety of surgical treatments during pregnancy with your doctor to decide whether to receive it after its full understanding.