For Patients
Introduction
Japan Society of Gynecologic Oncology is an academic organization run by gynecologists, pathologists, radiologists, and others who specialize in the diagnosis and treatment of gynecological tumors. This website describes current standard treatments for gynecologic tumors and relevant up-to-date information.
This website only describes standard treatments for gynecologic tumors. If you have any questions about your individual diagnosis and treatment, we recommend that you first consult with your doctor and ask for a second opinion at nearby hospitals where local gynecological oncologists are enrolled.
What is gynecologic tumor?
Human body consists of as many as approximately 60 trillion cells. Those cells disappear and are replaced by new cells after a certain period of time. For example, skin cells have a lifespan of 28 days, with old cells exfoliated and replaced by new skin cells. However, when those cells do not die and continue to grow for some reasons, a mass (swelling) called a tumor forms. Tumors include malignant tumors that metastasize to other organs or invade into surrounding area, and benign tumors that do not. Uterine myoma is considered a benign tumor because it is not metastatic or invasive even after they grow, while cervical cancer and uterine body cancer are malignant tumors because they are metastatic and invasive. It has been known that tumors are caused by genetic abnormalities.
The uterus and ovary are the organs of main focus in gynecology (Fig. 1). The uterus is an organ within the pelvis and its size in adult women is about that of a chicken egg. The uterus consists of the body and the cervix. The body of the uterus is composed of muscle with its inside covered by the endometrium. The endometrium repeats its proliferation and differentiation in association with menstrual cycles, and its detachment results in menstruation. Uterine myoma is a benign tumor that originates in the uterine muscle, and is the most common among benign tumors. Reflecting the tendency of late marriage, how the uterine myoma in unmarried women and infertility cases should be treated has recently become an issue.
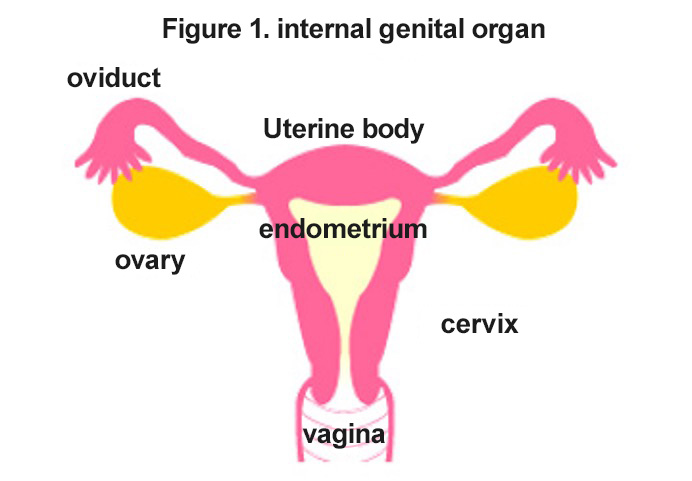
Malignant tumors that develop in the uterus are classified into two types: cervical cancer that develops in the cervix of the uterus, and uterine body cancer (also called endometrial cancer) that develops in the body of the uterus. These two types of cancer have completely different characteristics. Most cervical cancers are caused by persistent infection of human papillomavirus (HPV), while most uterine body cancers are caused by long-term stimulation by a female hormone called estrogen. Uterine body cancer is known to be more common in women with obesity, diabetes, and hypertension as well as those with fewer pregnancy and childbirth.
The ovary is an organ that produces and secretes female hormones and performs ovulation. One each is present in the right and left side of the pelvis. Its size is about that of thumb tip, but it shrinks to become smaller after menopause. Numerous types of tumors can develop in the ovary. Previously, ovarian cancer was common in Europe and the United States, but recently it is increasing in Japan as well. Multiple factors are involved in the development of ovarian cancer. Genetic factors are sometimes involved, represented by well-known "hereditary breast and ovarian cancer (HBOC)" due to alterations in the genes, BRCA1 and BRCA2.
Estrogen, one of female hormones, stimulates the growth of the endometrium and is involved in the development of uterine body cancer as well as endometrial hyperplasia, a precancerous lesion. Breast cancer also develops in association with female hormones. As mentioned above, "heredity" is one of the causes of breast cancer.
Recent Trends in Gynecologic Cancer
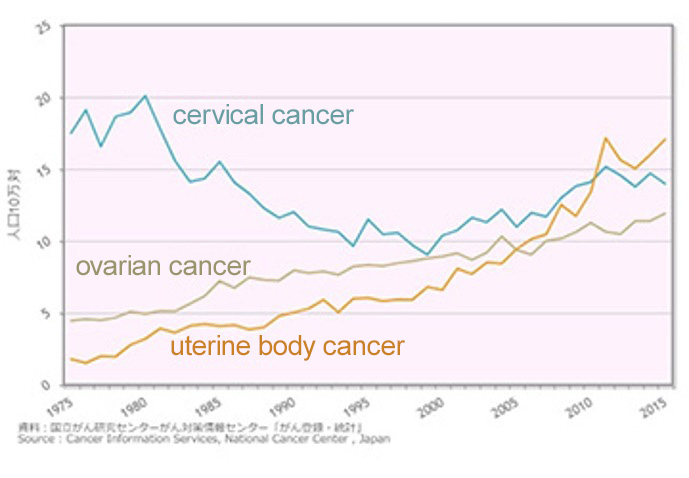
Prevalence of gynecologic cancer has changed in association with the changes in lifestyles (Fig. 2). The gynecologic cancers recently increasing in Japan are breast cancer, uterine body cancer, ovarian cancer, and cervical cancer among young women.
Cervical cancer is the most common among gynecological malignancies. The prevalence of cervical cancer is 0.29% among people in their 30s, 0.13% in their 40s, and 0.08% in their 50s, indicating that this cancer is common among younger women. Its early detection at the stage of dysplasia and the cancer in situ, which are precancerous lesions, leads to enabling the preservation of uterus. Human papillomavirus (HPV), which can be transmitted by sexual activity, is involved in the development of cervical cancer. National routine HPV vaccination is currently conducted for women aged 12-16 years, but the drastic decrease of its rate has become a social problem.
Uterine body cancer accounts for more than 30% of uterine cancers, and its incidence has more than doubled within this decade. The peak age of the onset of uterine body cancer, that is, 50s and 60s, is slightly older than that of cervical cancer.
Ovarian cancers are often found after they have advanced; however, new molecular targeting agents are beginning to be used for advanced or recurrent cancers, promising the improvement of their treatment outcomes.
The number of breast cancer cases has increased by 2.6 times in the last 20 years, representing an obviously continuing increase. Breast cancer is characterized by the peak of onset in the 40s and that of deaths in the 50s, and is now a leading cause of cancer mortality among women in late middle age. Breast cancer is generally considered to show better prognosis than other cancers, but it should be noted that it can recur long after receiving treatments. Early detection is important to reduce the mortality rate of breast cancer. The main symptom of breast cancer is a lump in the breast, which can be detected by yourself with careful palpation. However, some types of breast cancer do not form lumps or form only small lumps if any. In these cases, mammography (X-ray) and/or ultrasonography are used for their diagnosis.
Below, experts will discuss more details on these diseases and gynecological exam.
Figure 2. Annual trends in gynecologic cancer morbidity (age-adjusted morbidity, national estimate)